-
- Shozda, MSc in Nursing Science, Nursing School teacher, MUK, Karaganda, Kazakhstan
- Vaartio-Rajalin, Professor in gerontological care (tenure track), docent, Åbo Akademi University, Finland
ABSTRACT
Aim: The aim of this essay is to describe the reflextions concerning advanced nursing care for complex cardiologic conditions
Methods: a theoretical-reflective essay, conducted in a dialectical process between evidence-based literature, theoretical frameworks and reflection.
Results: The existing clinical nursing guidelines for cardiac rehabilitation integrate individual assessment and health education, psychosocial health, collaboration with caregivers and medical rehabilitation. However, they could be further developed: The Middle‐Range Theory of Self‐care of Chronic Illness could be applied into patient education and interaction between the patient-family-treatment team, and the nursing sensitive outcomes could be measured at the different phases of illness trajectory with interviews of patients, and quantified with PREMs (Patient Recorded Experience Measures) as well as PROMs (Patient Recorded Outcome Measures).
Keywords: Complex conditions, Advanced nursing care, Nursing theory, Cardiological patients
Advanced nursing care is vital especially in situations in which the patient suffers from a complex condition, i.e. multiple concurrent chronic conditions, functional and cognitive impairments, mental health challenges and social vulnerability [1]. The concept of complexity widens the scope of care to the person´s different care needs during the whole illness trajectory. These assessment and response responsibilities (in relation to perceived symptom clusters, perceived mental health, social vulnerability, functional capacity, knowledge expectations, self-care resources and quality of life) should be conducted in collaboration with the patient, with validated clinical questionnaires, and with focus on nursing sensitive care outcomes.
This essay is based on a course material received at EU-financed project AccelEd and the course “Nursing theories and research on patients with complex and long-term health needs” within it. In addition, articles and information were searched from databases CINAHL, PubMed, Web of Science. The complex condition chosen for this essay is a cardiological disease.
In a systematic review (n = 15) the most common perceived symptoms within cardiology are shortness of breath/difficulty breathing, sleep disturbance, edema, anxiety, chest/arm/jaw/back pain, nausea, dizziness, cognitive impairment, sweating, cough and weakness. In most studies, there were 6-14 symptoms evaluated. The number of symptom clusters (f.eg. combination of chest pain and shortness of breath), then, ranged 6-33. [2.] At the beginning of the illness trajectory a cardiologic patient usually has difficulties with common ADLs such as eating, toileting, dressing, taking medications, bathing, walking, and climbing stairs. Predictors of difficulty with ADL are female sex, not married, diabetes mellitus, cerebrovascular disease, dementia, morbid obesity, anemia, age (per 10-year increase). [3.] When patient arrives to emergency care, the most common symptoms are dyspnea, fatigue and edema. After stabilization of condition, patient usually perceives anxiety, sleep disorders and sadness. [4] Furthermore, patients with perceived physical limitations have obvious repercussions on their quality of life (higher levels of depression and anxiety, poorer physical, mental health and sexual relationships, higher distress, and lower adjustment to disease)[5].
Patient education is an evident part of advanced care. Due to the symptom clusters patients with cardiological diseases have knowledge expectations in relation to their own responsibility for the success of their care, medication’s costs, insurance, where to get for further care or treatment, and possible complications of the treatment. Important aspects of self-care capacity are f.eg. skills to take medications as prescribed, consult with doctor or nurse within possible deterioration of own condition, taking weigh daily, limiting fluid/salt intake, and exercising regularly. [6.] Some studies give strong support for educational interventions in relation to improved self-care skills [7] and quality of life [8] especially if intervention is based on a nursing theory [7].
The National Research Center for Health Development (http://www.rcrz.kz/) offers clinical nursing guidelines for cardiac rehabilitation. These recommendations integrate individual assessment and health education, psychosocial health, collaboration with caregivers and medical rehabilitation, but they could be further developed. The Middle‐Range Theory of Self‐care of Chronic Illness [9, 10] could be applied into patient education (see Figure 1) and interaction between the patient-family-treatment team. Furthermore, a self-report workbook for identifying patients’ knowledge expectations could be developed, for this method showed good results in oncologic context [11].
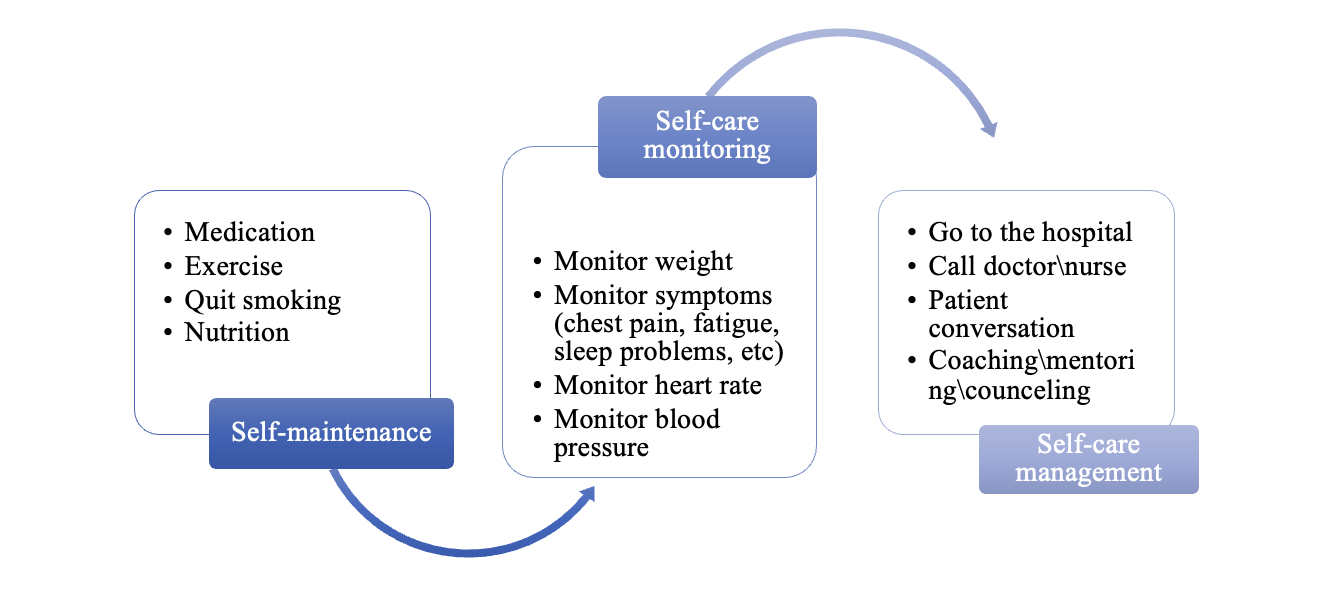 Figure 1. Application of The Middle‐Range Theory of Self‐care of Chronic Illness (Riegel et al. 2012, 2019) into patient education within a complex cardiologic condition
Figure 1. Application of The Middle‐Range Theory of Self‐care of Chronic Illness (Riegel et al. 2012, 2019) into patient education within a complex cardiologic conditionIf patient know more about his condition and get from nurse guiding and mentoring, it gives him feel of control in managing the condition and sense of security [12]. The anticipated nursing sensitive outcomes could be f.eg. sense of satisfaction, reduced anxiety, increased self-care ability, reduced readmission and improved quality of life. These outcomes could be measured at the different phases of illness trajectory with interviews of patients, and quantified with PREMs (Patient Recorded Experience Measures) such as CARE (Consultation and Relational Empathy) questionnaire [13] and practical issues of the hospital questionnaire [14]; and PROMs (Patient Recorded Outcome Measures) such as KCCQ (Kansas City Cardiomyopathy Questionnaire, [15]), MLHFQ (Measurement of Health-Related Quality of Life [16]) and condition specific questionnaires such as Beck´s scale of depression [17].
List of references
[1] Manning E, Gagnon M. (2017). The complex patient: A concept clarification. Nurs Health Sci 19, 13– 21. doi: 10.1111/nhs.12320. [2] A DeVon H, Vuckovic K, Ryan C, Barnason S, Zerwic J, Pozehl B, Schulz P, Seo Y, Zimmerman L. (2016). Systematic review of symptom clusters in cardiovascular disease. Eur Jour Cardiov Nurs 16(1), 6-17. https://doi.org/10.1177/1474515116642594 [3] Dunlay SM, Manemann SM, Chamberlain AM, Cheville AL, Jiang R, Weston SA, Roger VL. (2015). Activities of daily living and outcomes in heart failure. Circulation. Heart Fail 8(2), 261–267. https://doi.org/10.1161/CIRCHEARTFAILURE.114.001542 [4] Kurogi EM, Butcher RD, Salvetti MD. (2020). Relationship between functional capacity, performance and symptoms in hospitalized patients with heart failure. Rev Brasil de Enf 73(4), e20190123. https://doi.org/10.1590/0034-7167-2019-0123 [5] Serrano-Rosa MÁ, León-Zarceño E, Giglio C, Boix-Vilella S, Moreno-Tenas A, Pamies-Aubalat L, Arrarte V. (2021). Psychological State after an Acute Coronary Syndrome: Impact of Physical Limitations. Int J of Env Res Publ Health 18(12), 6473. https://doi.org/10.3390/ijerph18126473 [6] Ingadottir B, Thylén I, Jaarsma T. (2015). Knowledge expectations, self-care, and health complaints of heart failure patients scheduled for cardiac resynchronization therapy implantation. Patient Pref and Adh 9, 913–921. https://doi.org/10.2147/PPA.S83069 [7] Tok Yildiz F, Kaşikçi M. (2020). Impact of Training Based on Orem’s Theory on Self-Care Agency and Quality of Life in Patients With Coronary Artery Disease. J of Nurs Res 28(6), e125. https://doi.org/10.1097/JNR.0000000000000406 [8] Gomes L, Liébana-Presa C, Araújo B, Marques F, Fernández-Martínez E. (2021). Heart Dise ase, Now What? Improving Quality of Life through Education. Int J of Env Res Publ Health 18(6), 3077. https://doi.org/10.3390/ijerph18063077 [9] Riegel B, Jaarsma T, Strömberg A. (2012). A Middle-Range Theory of Self-Care of Chronic Illness. Adv Nurs Sci 35(3), 194–204. doi: 10.1097/ANS.0b013e318261b1ba [10] Riegel B, Jaarsma T, Lee CS, Strömberg A. (2019). Integrating symptoms into the Middle‐Range Theory of Self‐Care of Chronic Illness. Adv Nurs Sci 42(3), 206-215. https://doi.org/10.1097/ans.0000000000000237
[11] Vaartio H, Leino-Kilpi H, Puukka P. (2017). Development of a Self-Report Workbook for Identifying Cancer Patients Knowledge Expectations. The J of Nurs Care 6, 1-7. https://doi.org/10.4172/2167-1168.1000425 [12] Sanaie N, Kakhki AD, Ahmadi F. (2021). Exploring the consequences of patient commitment to cardiac rehabilitation program: A qualitative study. J of Educ and Health Prom 10, 30. https://doi.org/10.4103/jehp.jehp_828_20 [13] Mercer SW, Maxwell M, Heaney D, Watt GCM. (2004). The consultation and relational empathy (CARE) measure: development and preliminary validation and reliability of an empathy-based consultation process measure, Fam Pract 21(6), 699–705, https://doi.org/10.1093/fampra/cmh621. [14] Kingsley C, Patel S. (2017). Patient-reported outcome measures and patient-reported experience measures. BJA Education 17(4), 137-144. doi: 10.1093/bjaed/mkw060 [15] Spertus JA, Jones PG. (2015). Development and Validation of a Short Version of the Kansas City Cardiomyopathy Questionnaire. Circ Cardiovasc Qual Outcomes 8(5), 469-76. doi: 10.1161/CIRCOUTCOMES.115.001958. [16] Gordon HG. (1993). Measurement of Health-Related Quality of Life in Heart Failure. J Am Coll Cardiol 22, 185-9. doi: 10.1016/0735-1097(93)90488-m. [17] Beck AT, Ward C, Mendelson M. (1961). “Beck Depression Inventory (BDI)”. Arch of Gen Psych 4, 561-571. doi:10.1002/9781118625392.wbecp261
- Masters and PhD nursing students from Kazakhstan internship at European universities during AccelEd project
- International Scientific and Practical Conference
- Advanced nursing care of patients with chronic heart failure
- Advanced nursing care of patients with complex, cardiologic conditions
- Development of clinical thinking with a student a basis for risk management in practical activity of a health care worker
- Шиеленіскен жағдайлардағы мейіргерлік күтімге қатысты Кэтрин Колькабаның жайлылық теориясы
- Katie Eriksson’s theory of caritative caring
- Мейіргер ісінің мықты жақтары бар ма?
- Ковид-19 кезіндегі көшбасшылық
- Мейіргер ісіндегі көшбасшылық
- Лидерство в сестринском деле
- Distance education in nursing
- Leadership in times of Covid-19
- What is nursing management in practice?
- Is there a strong nursing vision?
+7172 539 533